The World Health Organisation says that health is a state of full physical, mental, and social well-being, not just the lack of illness or disease.
Hospitals, medical devices, clinical trials, outsourcing, telemedicine, medical tourism, health insurance, and medical equipment are all part of the healthcare business.
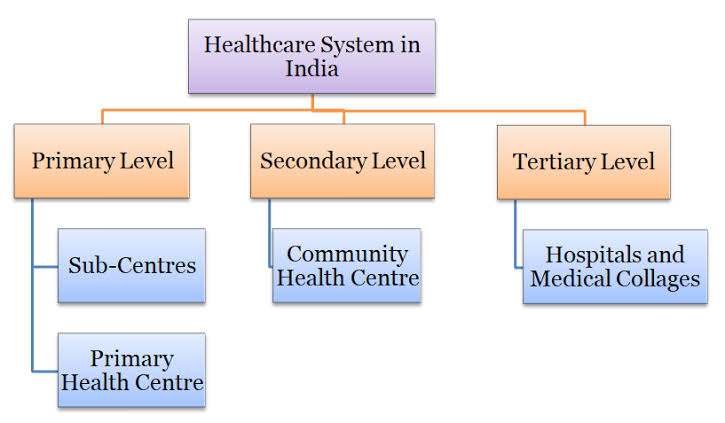
India’s health care system is made up of both state and private health service providers at the moment. Networks of basic, secondary, and tertiary health care facilities, which are mostly run by State Governments, offer free or very cheap medical care. There is also a large private health care industry, which includes everything from individual doctors and their clinics to general hospitals and super specialty hospitals.
Not enough medical staff: • There is a huge lack of medical staff, infrastructure, and connections to the last mile in rural places. g.: There are 1 doctor for every 1800 people, and 78% of them work in cities, where 30% of the people live.
• There are huge gaps in the supply of services (like people, hospitals, and diagnostic units in the private and public sectors), which are made worse by the fact that they aren’t available in the same way in all States or even in some of them.
• For example, even in a well-placed state like Tamil Nadu, government facilities are over 30% short of medical and non-medical workers.
• 61% of PHCs only have one doctor, and almost 7% don’t have any.
• Only 33% of PHCs have lab technicians, and only 20% have chemists.
• In places like Odisha, there are more than 3,000 empty government doctor jobs, which is about half of all government doctor jobs.
• India’s spending on health care has gone from 1.2% of GDP in 2013-14 to 4.0% of GDP in 2017-18. This is a small increase. This was supposed to be 2.5% of GDP, according to the National Health Policy for 2017.
• The health budget hasn’t grown in real terms, and there isn’t a plan to make the public and private sectors stronger in places where they are weak. Even though Ayushman Bharat makes health care portable, it is important to remember that it will take time for hospitals to be built in areas that need them. This could cause people to move to the southern states, which have better health care facilities than the rest of India.
Infrastructure problems: • There are questions about whether India’s infrastructure can handle the extra cases during pandemics like Covid-19.
• As a strategy, the government is trying to get more medical tourists and patients from other countries, as well as more insured and uninsured patients from their own country.
The country’s public health care system is falling apart, so most people have to go to private centres and hospitals.
• There aren’t enough PHCs (22%) and sub-health centres (20%), and only 12% of primary health centres and 7% of sub-health centres meet Indian Public Health Standards (IPHS).
• There aren’t many sub-centers or basic health centres in the northern states. The connection to a basic healthcare centre in the first mile is broken. For example, there is one PHC for every 28 towns in Uttar Pradesh.
Strong Role of Private Players: • About 70% of healthcare services in India are given by private players. If private healthcare falls apart because of money problems or other problems, India’s whole healthcare system could fall apart.
• More than 70% of all money spent on health care comes from the business sector.
• However, there aren’t enough private hospitals in Tier-2 and Tier-3 cities, and there’s a trend in Tier-1 places towards superspecialization.
• A lack of openness and bad behaviour in the private industry.
• The fact that public and private hospitals don’t have the same rules has been a big worry, especially since public hospitals would still get money from the government. This would make private players less likely to take part in a government plan.
High Out-of-pocket costs: • According to the latest National Health Accounts (NHA) figures, which came out in March 2021, patients pay up to 61% of the total cost of health care out of their own pockets.
• Even poor people have to choose private health care and pay for it out of their own money. Because of this, about 63 million people fall into poverty every year because of health costs.
• There are differences in health care because of many things, including geography, socioeconomic standing, and income groups, among others. India’s health care results aren’t as good as those of countries like Sri Lanka, Thailand, and China, which all started out at about the same level.
Not enough people have insurance:
• India has one of the world’s lowest health care costs per person. In the UK, the government pays about 83.5 percent of the cost of insurance. In the US, the government pays about 32 percent.
• The fact that 76% of Indians don’t have health insurance means that they have to pay a lot out of pocket for medical care.
Fake doctors: • Rural medical practitioners (RMPs), who provide 80% of outpatient care, have no official training for it.
• People fall for quacks, which can cause serious injuries or even death.
Numerous Schemes and Their Limits: • The government has started a lot of policies and health schemes, but only some of them have worked.
• The National Health Policy (NHP) of 2002 called for the government to spend 2%–3% of the gross domestic product (GDP) more on health care by 2010. This has not happened yet.
• Now, the 2017 National Health Policy wants to bring it up to 2.5% of the GDP by 2025.
• The National Health Mission, India’s flagship plan for primary health care, is still in a bad place overall.
• The NHM’s part of the health budget dropped from 73% in 2006 to 50% in 2019 because States didn’t raise their health spending in the same way and by the same amount.
Without a whole-person approach, healthcare:
• There are a lot of things that affect health that aren’t under the Health Ministry’s control, like better drinking water and sanitation, better diet, health, and education for women and girls, and safer roads and cleaner air.
Issues in particular with Urban healthcare
• Rural-urban disparity: Up until recently, the Union government focused mostly on health care in rural areas. Example: In 2019-20, 850 crore was spent on urban areas, while nearly 30,000 crore was spent on rural areas.
• Lack of basic and preventive health infrastructure on the part of the government: Only 5,190 of the norm-based goal of 9,072 urban primary health centres (UPHCs) are open.
• Most states don’t have urban sub-centres (SCs), which are the first place people go to get medical care. In cities, there are only 3,000 SCs, while there are more than 150,000 in rural places.
• Basic care that should be done in clinics is also “over-hospitalized” in cities.
• The state government doesn’t give out enough jobs, and the roles of the different health-related bodies aren’t clear enough.
• ULBs don’t have enough money, and health isn’t a high concern.
Issues in particular with Rural healthcare
• The Indian Public Health Standards (IPHS) are met by only 11% of sub-centers, 13% of Primary Health Centres (PHCs), and 16% of Community Health Centres (CHCs) in rural India.
• There is only one allopathic doctor for every 10,000 people, and there is only one state-run hospital for every 90,000 people.
• Patients or their family members who are innocent and can’t read or write are taken advantage of, and they aren’t told what their rights are.
• Most of the centres are run by paramedics who don’t have a lot of training or don’t have a lot of training at all. In rural areas, it’s hard to find a doctor.
• In an emergency, patients are sent to a tertiary care hospital, where a group of health workers and brokers can easily take advantage of them.
• One problem with India’s rural health care is that simple drugs aren’t always available.
• In many country hospitals, there aren’t as many nurses as they need to be.
Schemes from India’s central government for the health care sector
Health is a state responsibility. The Central Government helps the State Governments provide basic, secondary, and tertiary health care through a number of programmes.
• The Indian government wants to spend 2.5% of the country’s GDP on health care by 2025.
• The Union Budget 2020-21 gave more than Rs 65,000 crores to the Ministry of Health and Family Welfare.
• In fund 2020-21, the Indian government gave the National Health Mission a fund of around Rs 34,000 crores to keep going.
• The National Health Mission (NHM) helps pay for ASHA workers, ambulances, mobile medical units (MMUs), drugs and tools, and support for reproductive, maternal, newborn, child, and adolescent health (RMNCH+A).
• The goal of the National Nutrition Mission is to reduce undernutrition and stunting by 2%.
• The Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana (PMJAY) is the largest government-funded health care programme.
• PMJAY was given a fund of more than Rs 6400 crores in the Union fund for 2020-21.
• As of November 2019, more than 63 lakh people have been treated for free through the Ayushman Bharat – PMJAY programme.
• In the Union Budget for 2020-21, the Indian government gave Rs 3,000 billion to the Pradhan Mantri Swasthya Suraksha Yojana (PMSSY) programme.
India needs to take steps in the health field
• Public spending needs to go up right away to 2.5% of GDP, even though that’s less than the world average of 5.4%.
• A worry-free and all-encompassing health care system for everyone depends on how well health and wellness centres work. This is because they will help reduce the greater load of out-of-pocket health care costs.
• We need to stop the current trend of inconsistent and insufficient growth in health spending and put a lot of money into public health over the next ten years.
• A National Health Regulatory and Development Framework needs to be made to improve the quality, performance, fairness, effectiveness, and accountability of healthcare service across the country. For example, health practitioners need to be registered.
• Make more public-private partnerships to get health care to the last mile.
• There should be more generic drugs and Jan Aushadi Kendras to make medicines more cheap and cut down on the main part of Out of Pocket Expense.
• The government’s National Innovation Council, whose job it is to give healthcare experts, stakeholders, and other key players a place to work together, should promote a culture of innovation in India and help make policy on innovations that will focus on an Indian model for growth that benefits everyone.
• India should work towards Universal Health Coverage like other growing countries, like Thailand. UHC is made up of three parts: There is support for people, diseases, and costs.
• Using the benefits of IT, like e-health and m-health programmes based on computers and mobile phones, to improve the quality of health care services. From process automation to diagnostics to low-cost innovations, start-ups are putting money into the healthcare industry. To make health care available and affordable, there should be policy and regulation support.
The next step
• To solve problems in the healthcare business, India needs to look at the whole picture.
• This means that the public, private, and individual groups must all work together actively.
• Public spending needs to go up right away to 2.5% of GDP, even though that’s less than the world average of 5.4%.
• A worry-free and all-encompassing health care system for everyone depends on how well health and wellness centres work. This is because they will help reduce the greater load of out-of-pocket health care costs.
• We need to stop spending on health in a way that is inconsistent and not enough, and instead put a lot of money and time into public health over the next ten years.
• A National Health Regulatory and Development Framework needs to be made to improve the quality, performance, fairness, effectiveness, and accountability of healthcare service across the country. For example, health practitioners need to be registered.
• Make more public-private partnerships to get health care to the last mile.
Increase the number of generic drugs and Jan Aushadi Kendras to make medicines more affordable and reduce the major part of Out of Pocket Expenditure. The government’s National Innovation Council, which is supposed to provide a platform for collaboration between healthcare domain experts, stakeholders, and key participants, should encourage a culture of innovation in India and help develop policy on innovations that will focus on an Indian model for inclusive growth. UHC is made up of three parts: There is support for people, diseases, and costs.
• Using the benefits of IT, like e-health and m-health programmes based on computers and mobile phones, to improve the quality of health care services. From process automation to diagnostics to low-cost innovations, start-ups are putting money into the healthcare industry. To make health care available and affordable, there should be policy and regulation support.
• Using AYUSH services for care that isn’t life-threatening, as was shown during the pandemic, can be a key way to boost the capacity of allopathic services.
• To deal with the double disease burden, we need a more dynamic and proactive method.
• If everyone has access to health care, the country will be fit and healthy, which will help the country take advantage of the generational dividend.






 : International Relations | UPSC Notes")




 Marksheet, Notes, Strategy, Biography")



 : History, Funding, Contribution & Challenges")

